Canalicular Tear Repair
Canaliculi are mucosal ducts through which tears drain from the eye. The canalicular portion of the tear drainage system is located on the eyelids. The drainage system consists of the puncta on the upper lid and the lower lid, the canaliculi, the common canaliculus, the lacrimal sac, and the nasolacrimal duct. Tearing can result from the disruption of the lacrimal anatomy if the repair is not done immediately. Both inferior and the superior lacrimal drainage system are needed in proper functioning of the tear drainage system. Canalicular lacerations are most common in young adults.
When the laceration occurs to the canaliculus of the lacrimal system, both medial and lateral cut ends of the tear ducts are retracted due to its elasticity. If the laceration is close to the punctum, the medial canaliculus will be near the lid margin and a repair may be relatively simple. However, if a traumatic laceration occurs close to the lacrimal sac
The common canaliculus will be retracted deep into the medial canthal tendon and surrounding tissues. In this type of injury, the surgeon must look deeper for the medial canaliculus; and it can be very tedious to localize the medial cut end, which lies in deep tissues. The severed ends of the canaliculi should be repaired at the earliest. These procedures are best performed under general anesthesia. Proper anastomosis must be performed to recover proper function.
Causes of canalicular lacerations can occur by falls, trauma from a sharp object, motor vehicle accidents, scratches and sports trauma.
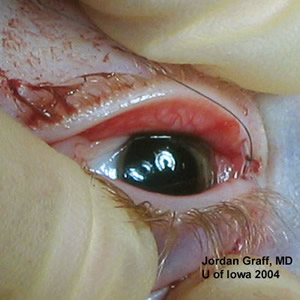
The puncta is dilated and a Bowman probe is passed delicately through the canaliculus. The severed end of the canaliculus is a shiny white cuff of tissue at the edge of the lumen. Intubation can be accomplished with either bicanalicular or monocanalicular intubation. The medial canthal tendon should also be repaired in its anatomic location, posterior to the lacrimal sac at the posterior lacrimal crest. If the disrupted tendon is not repaired, both the appearance and the function of the lid will be abnormal.
Patients with isolated canalicular trauma after they recover from anesthesia, may resume their preoperative diet. Normal activity can be resumed following surgery. Avoid blowing the nose as it can cause orbital emphysema. High-pressure activities that require Valsalva maneuvers should be avoided. Antibiotics will be given to help prevent infection. An ophthalmic antibiotic steroid often is used for topical use since it also decreases inflammation. Repairing canalicular lacerations can be complicated by difficulty in identifying and intubating the proximal injured system, retrieving stents in the nose, and repairing canalicular epithelium.