Pneumatic Retinopexy is an effective surgery for certain types of retinal detachments. A bubble of gas is used to push the retina against the wall of the eye, thus allowing fluid to be pumped out from beneath the retina. It is usually an outpatient procedure done with local anesthesia.
Procedure:
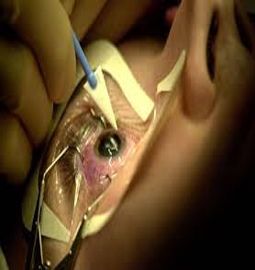
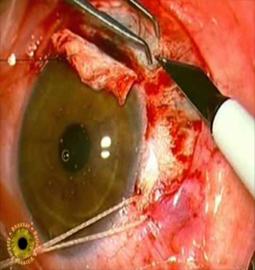
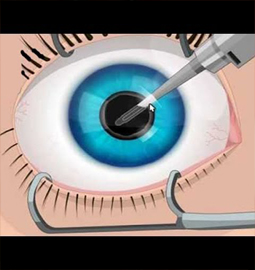
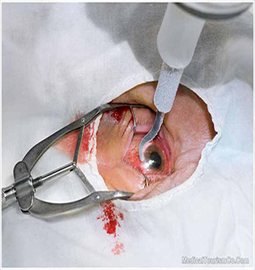
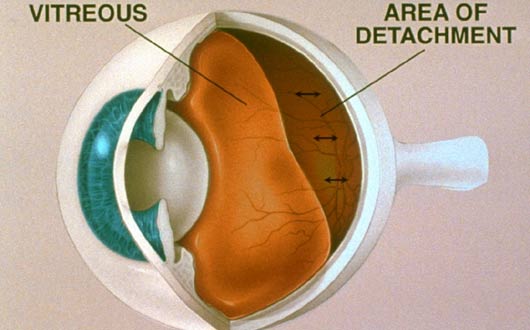
During pneumatic retinopexy, the eye doctor (ophthalmologist) injects a gas bubble into the middle of the eyeball. Your head is positioned so that the gas bubble floats to the detached area and presses lightly against the detachment. The bubble flattens the retina so that the fluid can be pumped out from beneath it. The eye doctor then uses a freezing probe (cryopexy) or laser beam (photocoagulation) to seal the tear in the retina.
A variation of this surgery uses a large bubble of silicone oil instead of a gas bubble to close and flatten the retina. A vitrectomy procedure, in which the vitreous gel is removed, is required to inject silicone oil. Because the silicone oil cannot be absorbed, a second procedure may be needed to remove the oil after the retinal detachment has healed.
A Fiber optic light source is used to illuminate and visualise the inside the eye during surgery. The surgeon would often use an infusion line to maintain the eye'x shape during surgery.Silicone oil or a gas (perfluropropane) is injected into the eye to replace the vitreous gel and restore normal pressure in the eye towards the end of the surgery.
Vitrectomy is always done by an eye doctor who has special training in treating problems of the retina.
Risks associated with it:
The most frequent problems from pneumatic retinopexy include:
The success of pneumatic retinopexy depends on keeping the gas bubble against the retina until it flattens. This will require you to hold your head and eye in the proper position for long periods of time.
Recovery tips:
Typically it takes about 3 weeks to recover from pneumatic retinopexy. It is very important to maintain the position of the gas bubble in the right place until a seal forms around the tear in the retina.
When silicone oil is used instead of gas, there may be less need to keep your head and eye in a precise position, because the oil bubble does not move as readily as a gas bubble. This may make the surgery and recovery easier for older adults, young children, and anyone who may have trouble keeping his or her head and eye in the proper position.
The location and size of a tear in the retina determines whether pneumatic retinopexy can be used. Pneumatic retinopexy can be useful when:
The break must be in the upper half of the eyeball for pneumatic retinopexy to be practical. You have to be able to position your head so that the break and the bubble are at the highest point. If the break was on the bottom of the eyeball, you would have to stay upside down during your recovery, which would not be practical.
A single treatment with pneumatic retinopexy reattaches the retina most of the time. With additional treatments such as vitrectomy or scleral buckling, the surgery is successful nearly all the time. Chances for good vision after surgery are higher if the macula was still attached before surgery. If the detachment affected the macula, good vision after surgery is still possible but less likely.
About Eye
Eye Diseases
Vision problems
Find Cost
Surgeries & Treatments
Best Eye Hospitals
Testimonials
Get Free Quotes
Top Hospitals In India
Top Hospitals In Turkey
Top Hospitals In Mexico
Top Hospitals In Costa Rica
Top Hospitals In Singapore
Top Hospitals In UAE
Top Hospitals In Australia
Top Hospitals In Malaysia
Top Hospitals In Thailand
Top Hospitals In Phillipines
Cataract Surgery
Intacs
Astigmatic Keratotomy(AK)
Canalicular Tear Repair
Chalazion Surgery
Conductive Keratoplasty(CK)
Corneal Transplantation
Lasik Surgery